
202461 Container lashing related MOB fatality while at sea
As edited from TSIB (Singapore) report TIB/MAI/CAS.065A container ship was underway at about 15 knots in an estuary, in daylight and good weather conditions, and approaching the pilot boarding station to pick up a pilot. The Master was alone on the bridge while almost all other crew (17 of 21), including a cook and a steward, were marshalled on deck to undertake container lashing removal. The arrival port’s stevedores did not habitually do unlashing tasks. While this task was not mandatory for the crew, it did offer extra pay for those who volunteered.
The volunteers were divided into four groups, each with a team leader. The second officer was team leader for Team 2.
At one point, the second officer was observed by another team member removing a vertical lashing rod from the third-tier container at the outermost row on the port side. The turnbuckle of the lashing rod had been removed and he was attempting to stabilise the rod. The lashing rod was 4.4m long and weighed 22.5kg. He was unable to control the rod and started swaying towards the ship’s side before falling through an unsecured gap into the sea 12.5m below, still holding the lashing rod. At that time, the vessel was making about 15 knots and was about two nautical miles from the pilot station.
The alarm was raised, and the man overboard (MOB) manoeuvre initiated. Although the Master released the bridge wing MOB life ring, the life ring did not pull the attached smoke-float off its support, and the smoke-float was left dangling in the air.
The nearby pilot boat that was bringing the pilot to the vessel started to search the area. The vessel’s crew attempted to launch their rescue boat, but the motor would not start. A lifeboat was then launched some 45 minutes after the accident. By now, other search and rescue (SAR) units were on scene as well. After over nine hours searching the victim was not found and presumed drowned.
The sea water temperature was about 6°C. In sea water of 5-10°C, unconsciousness is estimated to occur after about 30 minutes to one hour, with a survivability of about 1-3 hours depending on exhaustion levels.
Although the investigators were briefed on the roles of the persons involved, it was not possible to establish why the victim went to the outmost row and attempted to remove the outboard lashing rod. This role was to be performed only by persons wearing a safety harness attached to a strong point. The company’s personal protective equipment (PPE) matrix required crew members performing lashing and unlashing tasks at the outboard side to wear a safety harness which was to be tied to a lifeline. At the time of the incident, there were four sets of safety harnesses distributed to each team, and one person in each team had been assigned the safety harness.
The investigation found, among other things, that the victim had been sleeping before being called to perform the unlashing task, having come off watch five hours earlier. Although he had technically received enough rest according to international norms, it could not be ruled out that ‘sleep inertia’ might somewhat have affected his ability to assess the risk involved in handling the long and heavy rod near the ship side.
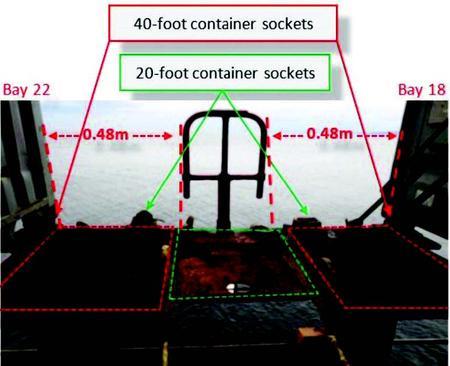
According to the company’s own risk assessment for this task, safety lines were to be rigged across the 0.48m gaps between bay 18 and 22 as a risk control measure to prevent falling overboard, yet there were no such safety lines rigged at these locations.
It is not routine for ship’s crew to perform lashing and unlashing of containers as these are historically and traditionally performed by stevedores. As such, if there is a need for the ship’s crew to perform such duties, it is important for any inexperienced crew to have physical hands-on practice under the supervision and guidance of experienced crew to assist them in appreciating the challenges and hazards they are likely to encounter.
Lessons learned
- This accodent is shockingly similar to that described in MARS 202460. Although in this case the company seemed to have a mature safety culture, 'procedural slip' and/or risk-taking was present. For example:
- Safety lines were not rigged at the openings between bat 18 and 22, contrary to the vessel's Safety Management Systtem (SMS);
- The victim disregarded his role as supervisor of Team 2 and proceeded to undertake a dangerous act (rouge behaviour);
- Other team members did not intervene to prevent the victim's unsafe act;
- Some crew unfamiliar with deck operations, such as the cook and steward, were nonetheless enrolled for the task.
Rescue and emergency equipment must be kept at 100% readiness because their reliability and functionality could be the difference between life and death.