
202254 - Fatal collapse of portable tween-deck
As edited from Dutch Safety Board report published December 2021
A small general cargo vessel in ballast was docked at port and crew were preparing to load various rice cargoes. As part of the preparations, temporary transverse bulkheads were installed and secured in both holds of the vessel. In the evening, an officer and two deckhands came on duty. Their task was to seal the gaps between the newly installed transverse bulkheads and the sides of the hold to prevent the different types of rice cargo from intermixing.
Starting at the top of the transverse bulkhead, the sealing procedure involved filling the gaps with sections of old ropes and then finishing with a strip of magnetic tape. This required working at height and lifting/shifting persons up and down in the hold. The hatchcover crane on board the vessel was equipped with electric winches and the vessel carried ‘man cages’ for this task. However, the crew found this way of working impractical, as the man cages were too small to transport enough old ropes for the task. Also, when pushing the ropes into the gap, the man cage often moves away from the bulkhead due to the reactionary force rather than providing an immovable platform. Instead, the smallest portable tweendeck was suspended from the two hoisting cables of the hatchcover crane and used as a working platform. This tweendeck weighs 20.2 tonnes, and has a width of 13 metres (the same width as the hold) and a length of more than 5 metres, which allows sufficient space to carry the necessary materials and tools. By lifting and lowering the tweendeck close against the bulkhead, crew members could stand on it and seal the gaps between the transverse bulkhead and the walls of the hold.
The use of the tweendeck as a work platform in this way had become part of the procedure described in the safety management system (SMS) for sealing gaps between walls of the hold and transverse bulkheads. This system was in place not only on the vessel in question, but in all similar vessels in the fleet. However, there was no specific description in the SMS on how the work should be carried out.
With the officer working the hatchcover crane and the two deck crew standing on the tweendeck, they began filling the gaps. Starting at the top of the hold, the tweendeck was gradually lowered in increments which allowed the deck crew to seal the gaps between the transverse bulkhead and the port and starboard hold walls.
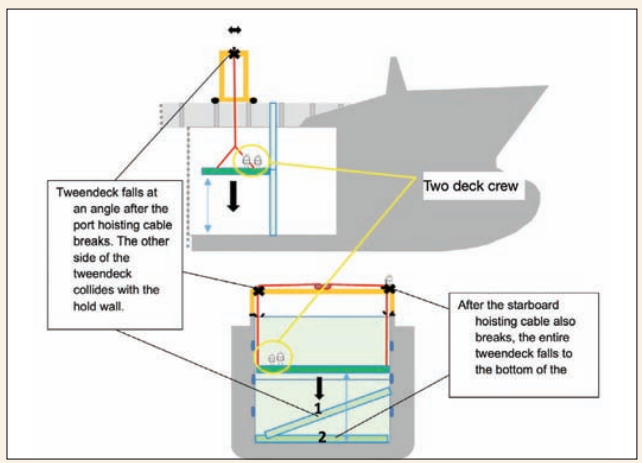
The port hoisting cable broke and the port side of the tweendeck fell to the bottom of the hold, damaging the starboard side of the hold wall and sending the two crew tumbling to one side. The starboard hoisting cable then also broke, and the entire tweendeck fell to the bottom of the hold.
As neither of the deck crew were wearing fall protection, both fell with the tweendeck. One was trapped between the port hold wall and the tweendeck. He died at the scene. The other deckhand suffered serious injuries and was transported to a shore hospital. He was subsequently repatriated. Following the occurrence, three safety harnesses were discovered stacked on the tweendeck.
Investigation revealed that both the port and starboard hoisting cables were extremely worn. Neither of them was well coated with lubricating grease to protect against the corrosive maritime environment.
The ‘safety coefficient’ or safety factor applied to the hoisting cables was 1:5, which is standard for lifting cargo or other loads such as the hatch covers but not for lifting persons, which is usually applied at a 1:10 ratio, or twice as stringent. The hoisting cables had been installed five years earlier and had been successfully tested and examined by a certification body about four years earlier. About nine months before the occurrence they had undergone and passed an annual examination.
Despite the fact that tweendecks were regularly used as a work platform at height, an activity that involved safety risks, no specific instructions were drawn up nor risk assessments carried out for working with tweendecks in this way.
The manual for the hatchcover crane did include checklists for maintenance and inspection. However, these checklists were not used and were not fully integrated in the compulsory operational maintenance routine (PMS) on the vessel. There was no other link between the PMS and the original manual for the hatchcover crane.
Editor’s note: The lessons learned that we have culled from the report can be seen in the light of several ‘safety issue’ categories;
Working at height issues
It appears the crew were informed and concerned about working at height, as safety harnesses had been fetched and were found on the tweendeck. However, they were not actually used.
- When working at height, always, always wear a safety harness and line that is rigged to protect from a fall.
- Appliances and accessories for lifting humans are usually specially designed for this purpose. The safety factors involved in the design and specifications are normally greater than those used for cargo.
Maintenance and inspection issues
- The wire rope was extremely worn. Cost cannot be a factor for not replacing a wire rope, because good products are readily available and are relatively inexpensive when compared to other vessel costs. In essence, there is no excuse for an old wire rope to be in use.
- Even new wires can be damaged at any time. Careful and regular inspections should be the norm, as should proper maintenance such as lubrication – preferably the penetrating type that goes to the wire rope core and leaves the exterior layer clear for proper inspection.
- As a good practice, companies should strive to integrate manufacturer’s specifications and advice for equipment used on their vessels into their SMS procedures.
Management of change issues
An alternative work method for sealing temporary transverse bulkheads in the hold had been developed. The use of a portable tweendeck as a work platform appeared to be a better solution than the use of man cages. But there were risks associated with this practice that had gone undetected because it appears proper risk assessments were not conducted prior to adopting the new work method. Any new procedure should be rigorously studied and risk assessments applied.