
202107 Fatigue and weak bridge practices contribute to expensive accident
As edited from NTSB (USA) report MAB 1908
A partially loaded bulk carrier was inbound in a port channel under pilotage. A rudder angle indicator was lit and, because the bridge had been darkened for night vision, it could easily be seen by the bridge team. The pilot conned the vessel from the centreline windows, the helmsman was directly behind him and the OOW was near the engine order telegraph just to the helmsman’s left.
Upon reaching a planned course alteration point the pilot gave a port 20-degree command to start the turn. The helmsman answered, ‘Port 20,’ but instead put the helm 20 degrees to starboard. About 11 seconds later the pilot saw that the wrong helm direction had been applied so he ordered ‘midships’ then repeated the port-20 order. Combined with a full-ahead burst of speed the vessel’s swing to starboard was arrested about 38 seconds after the original command to port had been given and the vessel regained the required heading.
Following the helmsman’s error and recovery, the pilot and OOW had a brief conversation about the mate’s duty to watch the helmsman. The second mate agreed to double-check the helmsman with each command. The Master was not on the bridge at the time. The OOW offered to call him, but the pilot declined. Although the OOW did not understand conversational English, he told investigators he understood the pilot’s orders.
Some 90 minutes later the vessel approached a major turn to starboard. By now the Master was on the bridge. The pilot planned to
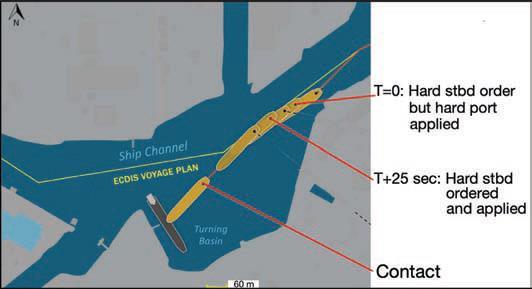
turn wide, intending to stay to the south side of the channel to pass a working dredger. The pilot gave a port 20-degree command to bring the ship slightly left, ahead of the turn to starboard, and the helmsman answered accordingly. The pilot’s next order to make the turn to the right, 24 seconds later, was ‘hard starboard’. The helmsman repeated the pilot’s order but instead put the rudder hard to port.
Ten seconds later, the pilot recognised the error and ordered midships while tapping with his fingers on the rudder angle indicator above his head to get the helmsman’s attention. It took the steering gear 15 seconds to shift from hard port to midships, and then the pilot repeated his original hard-starboard order. The rudder reached hard starboard 12 seconds later, although the ship’s heading was still falling to port at about 12 degrees per minute. The pilot now realised an emergency manoeuvre was needed.
The pilot ordered ‘Stop engines; let go anchor’ and seven seconds later, ‘full astern’. The vessel’s whistle was sounded. At this point the
vessel was making about 6 knots and its heading was still falling to port. The pilot estimated that increasing the engine speed to power through the turn, as he had done earlier, would not work so he chose instead to attempt to stop the vessel.
With the port anchor and two shots of chain deployed, the vessel nonetheless collided with the port side of a berthed tank barge while
making almost 4 knots. Although there were no fatalities or injuries as a result of this accident, the two vessels and the shore facility suffered damage that amounted to more than $21 million in total.
The investigation found, among other things, that the helmsman had probably been fatigued by carrying out extra duties the day before and that this contributed to the accident.
Lessons Learned
- When in restricted waterways the helmsman’s actions should always be verified by same-time sighting of the rudder angle indicator. A wrong rudder application may be irrecoverable if left for even 10 seconds.
- The OOW was apparently not sighting the indicator at all and, if he was, he did not indicate the wrong rudder application to the pilot. The pilot was sighting the rudder indicator but only after a 10- or 11-second delay. In the first instance they were able to recover, but not in the second.
- The work-rest log did not indicate the helmsman’s extra duties the day before. When collecting data for fatigue, investigators should not restrict themselves to looking at the work-rest logbooks, but should also question each person in detail about their previous 72-hour, or preferably 96-hour, work-rest routine.
Editor’s note: See the July 2013 Seaways article about investigating
for fatigue. The article can be found online at: http://safeship.ca/
uploads/3/4/4/9/34499158/investigating_for_fatigue_-_seaways_
july13.pdf